The post Curbing disease transmission through genetically modified mosquitoes appeared first on Awaam India.
]]>Mosquitoes are some of the most deadly creatures on the planet. They carry viruses, bacteria and parasites, which they transmit through bites, infecting some 700 million people and killing more than 1 million each year.
With international travel, migration and climate change, these infections are no longer confined to tropical and subtropical developing countries. Pathogens such as West Nile virus and Zika virus have caused significant outbreaks in the United States and its territories that are likely to continue, with new invasive pathogens being discovered all the time. Currently, control of these diseases is mostly limited to broad-spectrum insecticide sprays, which can harm both humans and non-target animals and insects. What if there was a way to control these devastating diseases without the environmental problems of widespread insecticide use?

Wilfredo Lee / AP Photo
Genetically modifying mosquitoes to prevent disease may sound like science fiction, but the technology has advanced in recent years to the point where this is no longer a scenario relegated to late-night movies. In fact, it’s not even a new idea; scientists were talking about modifying insect populations to control diseases as early as the 1940s. Today, genetically modified (GM) mosquitoes, developed during the past several decades of research in university laboratories, are being used to combat mosquito-borne pathogens – including viruses such as dengue and Zika – in many locations around the globe, including the United States. Progress is also being made to use GM mosquitoes to combat malaria, the most devastating mosquito-borne disease, although field releases for malaria control have not yet taken place.
I have been working on GM mosquitoes, both as a lab tool and to combat disease, for over 20 years. During that time, I have personally witnessed the technology go from theoretical, to seeing it used in the field. I’ve seen older techniques that were inefficient, random and slow pave the way for new methods like CRISPR, which enables efficient, rapid and precise editing of mosquito genomes, and ReMOT Control which eliminates the requirement for injecting materials into mosquito embryos. These new technologies make GM mosquitoes for disease control not a question of “if,” but rather a question of “where” and “when.”
Don’t worry, these genetic changes only affect the mosquitoes – they are not transmitted to people when the mosquito bites them.
Ways to use genetically modified mosquitoes

Achmad Ibrahim / AP Photo
There are two alternative methods currently used to control mosquito-borne diseases using GM mosquitoes. The first is “population replacement” in which a mosquito population biologically able to transmit pathogens is “replaced” by one that is unable to transmit pathogens. This approach generally relies on a concept known as “gene drive” to spread the anti-pathogen genes. In gene drive, a genetic trait – a gene or group of genes – relies on a quirk on inheritance to spread to more than half of a mosquito’s offspring, boosting the frequency of the trait in the population.
The second approach is called “population suppression.” This strategy reduces mosquito populations so that there are fewer mosquitoes to pass on the pathogen.
While the concept of gene drive in mosquitoes is many decades old, the gene-editing technique CRISPR has finally made it possible to easily engineer it in the laboratory. However, CRISPR-based gene drives have not yet been deployed in nature, mostly because they are still a new technology that lacks a firm international regulatory framework, but also due to problems related to the evolution of resistance in mosquito populations that will stop the gene from spreading.
It may not be immediately obvious, but the gene in “gene drive” need not be a gene at all – it can be a microbe. All organisms exist not just with their own genomes, but also with the genomes of all their associated microbes – the “hologenome.” Spread of a microbial genome through a population by inheritance can also be thought of as gene drive. By this definition, the first gene drive that has been deployed in mosquito populations for disease control is a bacterial symbiont known as Wolbachia. Wolbachia is a bacterium that infects up to 70 percent of all known insect species, where it hijacks the insect reproduction to spread itself through the population.
Thus, the Wolbachia itself (with its genome of approximately 1,500 genes) acts as the genetic trait that is driven into the population. When Wolbachia is transferred into a previously uninfected mosquito, it often makes the mosquito more resistant to infection with pathogen that can cause disease in humans, such as multiple viruses (including dengue and Zika viruses) and malaria parasites.
A bacterium that fights disease

Lynne Sladky/AP Photo
In the last eight years, researchers have taken Wolbachia present in fruit flies and transferred that bacteria into mosquitoes that transmit dengue virus. Those modified insects were then released in a dozen countries to control the disease. Although marketed as a “non-GM strategy,” artificially infecting mosquitoes with Wolbachia clearly falls under the GM umbrella, as over 1,500 genes (the entire bacterial genome) have been transferred from the original fruit fly host into the mosquitoes.
Preliminary dengue control results from these releases in Australia have been promising. However, control of the disease in other release areas with higher disease risk, such as South America and Asia, still needs to be determined, particularly as some studies have demonstrated that Wolbachia can sometimes increase pathogen infection in mosquitoes rather than suppress it.
GM mosquitoes that eliminate mosquitoes

Jason Rasgon, CC BY-ND
The best current example of population suppression is the release of genetically modified sterile mosquitoes. This is a modern spin on the decades-old Sterile Insect Technique (SIT), where sterile male insects are released into natural populations to mate with the wild females, reducing the mosquito population. But, rather than crudely sterilizing mosquitoes with radiation or chemicals, clever genetic engineering is now used to sterilize them instead. The company Oxitec has engineered mosquitoes with a gene that is lethal to females but not to males, which do not bite or transmit disease. Thousands of these transgenic males are released into nature, where they mate with the wild females in the population. The genetic modification is inherited by the offspring of these matings; female offspring die, while male offspring, which carry the gene, survive and continue passing the trait to further generations. With fewer and fewer females the mosquito population is drastically suppressed. Oxitec has conducted releases in the Grand Caymans, Malaysia, Brazil, and Florida.
There has been some opposition to these sterile mosquito releases, particularly in Florida. For example, in 2016, an Oxitec trial in the Florida Keys was met with some local resistance. However, unlike gene drive strategies, release of sterile mosquitoes (genetically modified or not) has about the smallest environmental footprint and highest safety of any disease control strategy; certainly safer than broad-spectrum insecticide sprays. It is highly targeted, and thus if it works, will only result in elimination of the target mosquito species, which in this case (Aedes aegypti) is a highly invasive and non-native mosquito in Florida.
In addition to gene drive, Wolbachia bacteria have also been used for population suppression. Males infected with the bacteria are released into a mosquito population that is either not infected, or infected with a different Wolbachia strain, which leads to “incompatible” or sterile matings. This strategy again has a long history, and was first used to suppress mosquito populations in the 1960s before people even knew that Wolbachia was causing certain populations of mosquitoes to be sterile when mated with one another. In current times, Wolbachia-sterilized males have been released in multiple countries including Australia and the U.S., in California and Florida, to control dengue virus.
In an increasingly interconnected world, and with the added problems of global climate change, pathogens are not likely to stay confined to the developing world, but will be an increasing issue for the U.S. as well. With the evolution of insecticide resistance in mosquitoes a certainty, GM technology has the potential to reduce the burden of mosquito-borne diseases across the globe, without the environmental and health risks associated with harmful pesticide use.
Don’t be afraid if it sounds like science fiction; it may just save your life.
Jason Rasgon, Professor of Entomology and Disease Epidemiology, Pennsylvania State University
This article was originally published on The Conversation.
The post Curbing disease transmission through genetically modified mosquitoes appeared first on Awaam India.
]]>The post When we lose weight, where does it go? appeared first on Awaam India.
]]>The world is obsessed with fad diets and weight loss, yet few of us know how a kilogram of fat actually vanishes off the scales.
Even the 150 doctors, dietitians and personal trainers we surveyed shared this surprising gap in their health literacy. The most common misconception by far, was that fat is converted to energy. The problem with this theory is that it violates the law of conservation of matter, which all chemical reactions obey.
Some respondents thought fat turns into muscle, which is impossible, and others assumed it escapes via the colon. Only three of our respondents gave the right answer, which means 98% of the health professionals in our survey could not explain how weight loss works.
So if not energy, muscles or the loo, where does fat go?
Read more:
Food v exercise: What makes the biggest difference in weight loss?
The enlightening facts about fat metabolism
The correct answer is that fat is converted to carbon dioxide and water. You exhale the carbon dioxide and the water mixes into your circulation until it’s lost as urine or sweat.
If you lose 10kg of fat, precisely 8.4kg comes out through your lungs and the remaining 1.6kg turns into water. In other words, nearly all the weight we lose is exhaled.
This surprises just about everyone, but actually, almost everything we eat comes back out via the lungs. Every carbohydrate you digest and nearly all the fats are converted to carbon dioxide and water. The same goes for alcohol.
Protein shares the same fate, except for the small part that turns into urea and other solids, which you excrete as urine.
The only thing in food that makes it to your colon undigested and intact is dietary fibre (think corn). Everything else you swallow is absorbed into your bloodstream and organs and, after that, it’s not going anywhere until you’ve vaporised it.
Kilograms in versus kilograms out
We all learn that “energy in equals energy out” in high school. But energy is a notoriously confusing concept, even among health professionals and scientists who study obesity.
The reason we gain or lose weight is much less mysterious if we keep track of all the kilograms, too, not just those enigmatic kilojoules or calories.
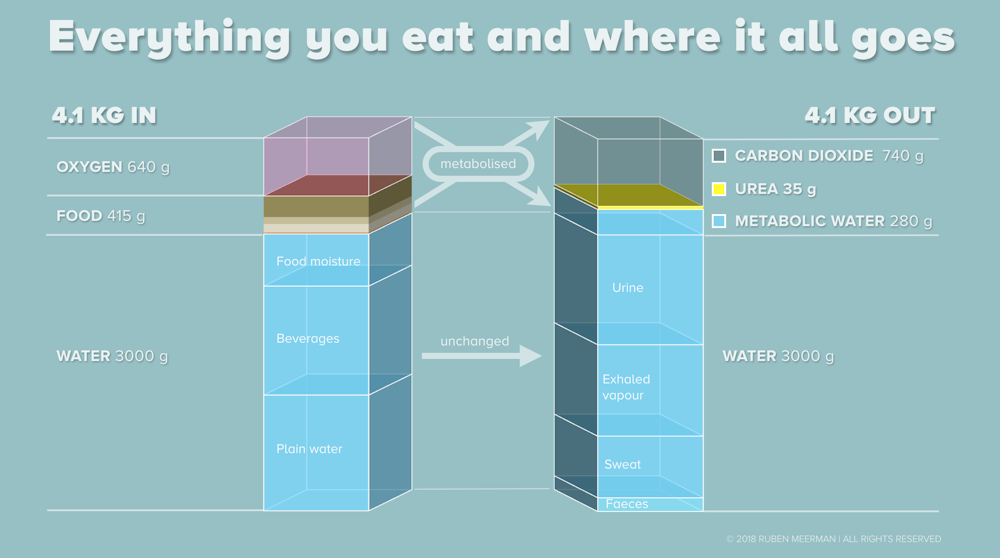
According to the latest government figures, Australians consume 3.5kg of food and beverages every day. Of that, 415 grams is solid macronutrients, 23 grams is fibre and the remaining 3kg is water.
What’s not reported is that we inhale more than 600 grams worth of oxygen, too, and this figure is equally important for your waistline.

from www.shutterstock.com
Read more:
Why we regain weight after drastic dieting
If you put 3.5kg of food and water into your body, plus 600 grams of oxygen, then 4.1kg of stuff needs to come back out, or you’ll gain weight. If you’re hoping to shed some weight, more than 4.1kg will have to go. So how do you make this happen?
The 415 grams of carbohydrates, fats, protein and alcohol most Australians eat every day will produce exactly 740 grams of carbon dioxide plus 280 grams of water (about one cup) and about 35 grams of urea and other solids excreted as urine.
An average 75kg person’s resting metabolic rate (the rate at which the body uses energy when the person isn’t moving) produces about 590 grams of carbon dioxide per day. No pill or potion you can buy will increase that figure, despite the bold claims you might have heard.
Read more:
Five supplements that claim to speed up weight loss – and what the science says
The good news is that you exhale 200 grams of carbon dioxide while you’re fast asleep every night, so you’ve already breathed out a quarter of your daily target before you even step out of bed.
Eat less, exhale more
So if fat turns into carbon dioxide, could simply breathing more make you lose weight? Unfortunately not. Huffing and puffing more than you need to is called hyperventilation and will only make you dizzy, or possibly faint. The only way you can consciously increase the amount of carbon dioxide your body is producing is by moving your muscles.
But here’s some more good news. Simply standing up and getting dressed more than doubles your metabolic rate. In other words, if you simply tried on all your outfits for 24 hours, you’d exhale more than 1,200 grams of carbon dioxide.
More realistically, going for a walk triples your metabolic rate, and so will cooking, vacuuming and sweeping.
Metabolising 100 grams of fat consumes 290 grams of oxygen and produces 280 grams of carbon dioxide plus 110 grams of water. The food you eat can’t change these figures.
Therefore, to lose 100 grams of fat, you have to exhale 280 grams of carbon dioxide on top of what you’ll produce by vaporising all your food, no matter what it is.
 Any diet that supplies less “fuel” than you burn will do the trick, but with so many misconceptions about how weight loss works, few of us know why.
Any diet that supplies less “fuel” than you burn will do the trick, but with so many misconceptions about how weight loss works, few of us know why.
Ruben Meerman, Assistant scientist, UNSW and Andrew Brown, Professor and Head, School of Biotechnology and Biomolecular Sciences, UNSW
This article was originally published on The Conversation. Read the original article.
The post When we lose weight, where does it go? appeared first on Awaam India.
]]>The post Why do our veins look blue when our blood is red? appeared first on Awaam India.
]]>This is an article from I’ve Always Wondered, a series where readers send in questions they’d like an expert to answer. Send your question to [email protected]
I’ve always wondered why our veins are blue, when blood is red? – Alexandra, 28, Melbourne
Blood is red, and a surgeon will tell you our veins too are red, they only look blue when we see them through our skin. But why?
The answer depends on a number of things, including how your eyes perceive colour, how light behaves when it contacts your body, and the special properties of blood.
Light travels in peaks and troughs. And the distance between each trough is called a wavelength. Different colours of light have waves of different lengths. Red light has a long wavelength (about 700 nanometres), violet light has a short wavelength (about 400 nanometres), and the rest of the spectrum is spread out in between.
We see something as a particular colour when light of that colour hits our eyes –either directly from a light source or reflected from a surface.
To understand what colour our veins appear, we need to think about what happens to different wavelengths of light when they hit our skin, how far they can travel through our skin, and what happens when they get to our veins.
Read more:
Curious Kids: Why are rainbows round?
The light that hits our skin during the day is basically white, which is a mixture of all the visible wavelengths. But to explain why our veins look blue, we will look at just the red and blue ends of the spectrum.
Red light has a long wavelength – and this means it is less likely to be deflected by materials and can more easily travel through. Red light can travel pretty well through the skin and body tissues, reaching up to 5-10mm below the skin, which is where many veins are.
When it gets to the veins, the red light is absorbed by the haemoglobin (the protein that makes our blood red). You can demonstrate this to yourself. If you shine a red light on your arm, you will see some red light reflected back, and dark lines where the veins are, as the red light is absorbed by the haemoglobin.
Read more:
Explainer: what’s actually in our blood?
Red light makes our veins appear as dark lines.
This phenomenon is actually used to help medical personnel find veins to take blood – by shining red, and sometimes infrared (which is an even longer wavelength) light on the arm.
Blue light has a short wavelength (about 475 nanometres), and is scattered or deflected much more easily than red light. Because it’s easily scattered it doesn’t penetrate so far into the skin (only a fraction of a millimetre). When blue light hits the skin, it’s mostly deflected back.
If you shine a blue light on your skin, what you see is basically blue skin, and veins are hard to find. You may have seen blue light used in spaces such as public bathrooms to discourage intravenous drug use.

Wikimedia Commons
{kind=link}
So, now imagine the red light and the blue light shining on your skin at once, as happens when you are under white light. You will have a mixture of red, blue and other colours reflected back where there are no veins. Where there are veins, you will see relatively less red, and relatively more blue compared to the surrounding skin.
This means your veins will appear blue compared to the rest of your skin.

Interestingly, the effect varies depending on how deep the vein is, and also on how thick the vein is. Very narrow veins close to the surface, such as the capillary bed, will not appear blue.
Blue veins appear more prominent in very pale skinned people, and this may have given rise to the expression “blue blood” for European nobility in the 19th century. These people were untanned from manual labour, and so their veins appeared blue under the skin.
With thanks to Science Writer at the Australian Red Cross Blood Service Alison Gould.
 * Email your question to [email protected]
* Email your question to [email protected]
* Tell us on Twitter by tagging @ConversationEDU with the hashtag #alwayswondered, or
* Tell us on Facebook
David Irving, is Adjunct Professor at University of Technology Sydney
This article was originally published on The Conversation.
The post Why do our veins look blue when our blood is red? appeared first on Awaam India.
]]>The post Why we should pay people to stop smoking appeared first on Awaam India.
]]>Despite some of the strictest tobacco control policies in the world, recent data shows the decline in smoking in Australia has stalled.
“First-line” quitting strategies available in Australia such as nicotine patches offer around a 7% success rate (or 93% failure rate, depending on how you look at it). This will not achieve our 9% smoking target by 2020, given that we are at about 14% now.
With current approaches and policies adopted in Australia having arguably lost their edge, and with more controversial approaches such as e-cigarettes caught up in political quicksand, let’s invest in the strategies that do work.
One evidence-based approach that has not received much attention in Australia is using financial incentives. Incentives programs reward quitters for not smoking by giving them a monetary voucher. The quitter’s abstinence is verified using biochemical tests of either their saliva, urine or breath.
What’s the evidence for financial incentives?
Financial incentive programs are one of the most effective and cost effective strategies for getting people to quit. They are considered the most effective strategy for pregnant smokers. They are also cost effective, with the calculated net benefit (after taking into account of the incentives used) being around A$4,300 per smoker, per attempt to quit. There have been a number of studies showing their benefits.
Using a multinational company as a test site, a team of US researchers found people who were offered US$750 (A$938) to quit smoking were three times more successful than those who were not given any incentives. Even six months after the vouchers had stopped, previously incentivised quitters were 2.6 (21.9% vs 11.8%) times more likely to still be smoke-free compared to non-incentivised quitters.
A team of UK researchers randomised over 300 pregnant women to receive up to £400 (A$661) worth of shopping vouchers if they quit during the pregnancy. Again, women in the incentives group were 2.6 (22.5% vs 8.6%) times more likely to have stopped smoking at the end of pregnancy, compared to the women who had received counselling and nicotine replacement therapy.
A Swiss program, offering low-income smokers up to US$1,650 (A$2,063) worth of quit-contingent vouchers staggered over six months, found smokers were 1.6 (18.2% vs 11.4%) times more likely to be smoke-free at 18 months compared to non-incentivised smokers.
In Australia, there are approximately 2.6 million adult daily smokers, who have been estimated to cost the government A$31.5 billion in social, health and economic costs each year. That’s about A$12,000 per smoker, which is much more than incentive programs offer.
Why does it work?
Quitting is hard – ask any smoker. Not only are the benefits, like other health behaviour changes, not immediate, but quitting smoking requires the smoker to go through a nasty period of withdrawal, while knowing the withdrawal symptoms could be immediately relieved by smoking.
Unlike other quit smoking programs using one or a combination of strategies (counselling, nicotine replacement therapy), incentives-based programs give the quitter the autonomy to choose the quit strategy that best suits them, and simply rewards them for their success. Importantly, incentives programs provide instant positive rewards for quitting.

Toa Heftiba/Unsplash
This phenomenon is described by behavioural economics as “temporal discounting”; a process explaining how humans have a preferential bias towards immediate reinforcement over delayed reinforcement, even if the delayed rewards are more valuable. Incentives therefore motivate quitters to stay on track in those difficult first few weeks of quitting smoking.
So why don’t we do it?
A common criticism of this type of intervention is that the targeted behaviour change is only maintained while the incentive is in place. Not only have incentives programs demonstrated long-term (one to two years) effectiveness superior to other treatment options, but even short-term behaviour change has important health implications.
Others are concerned people will “game” the program (say they’ve stopped smoking when they haven’t, or abstain from smoking just before verification). But research suggests this occurs in less than 5% of cases. After all, the majority of smokers actually want to quit.
Coersion and the ethical conundrum of free choice has been raised as an issue, with the concern that people will feel forced to sign up as they’ll be financially better off. But with a packet of cigarettes costing on average A$25 in Australia, the financial advantage of quitting seems to far outweigh the token financial incentive offered by such programs.
Finally, people have voiced their disapproval of a program that seemingly “rewards people for their bad behaviour”. Given the government subsidises medication to treat lifestyle-causing chronic conditions; it could be argued that this is much the same thing.
 Tobacco control should not be about blaming and shaming people for a decision they made years ago that’s resulted in a life-threatening habit. It’s about reducing the devastating health and economic impact of tobacco smoking by adopting strategies that are proven to be safe and effective.
Tobacco control should not be about blaming and shaming people for a decision they made years ago that’s resulted in a life-threatening habit. It’s about reducing the devastating health and economic impact of tobacco smoking by adopting strategies that are proven to be safe and effective.
Mai Frandsen is Postdoctoral Research Fellow at University of Tasmania Australia
This article was originally published on The Conversation. Read the original article.
The post Why we should pay people to stop smoking appeared first on Awaam India.
]]>